This website is under construction. Please visit after a week for the complete website experience.
Paediatric Surgery, Shaikh Zayed Hospital, Lahore

Anorectal Malformation
Contents
-
Examination Video
Basic Embryology & Anatomy
In the early embryo, the hindgut ends in a common chamber called the cloaca.
The cloaca is a single cavity that will later divide into:
-
an anterior urinary part
-
a posterior bowel part

A mesodermal partition called the urorectal septum grows downward between the future urinary tract and the future rectum.
Its job is to divide the cloaca into two parts.

By about the 7th week, the urorectal septum reaches the cloacal membrane and divides the cloaca into:
-
Anterior primitive urogenital sinus
-
Posterior anorectal canal

So now:the anterior part forms bladder and urethral structuresthe posterior part forms rectum and upper anal canal
The anal canal has two embryologic origins:
Upper part
-
comes from endoderm
-
derived from hindgut
Lower part
-
comes from ectoderm
-
derived from the proctodeum (anal pit)

The anal membrane normally breaks down, creating the external anal opening.
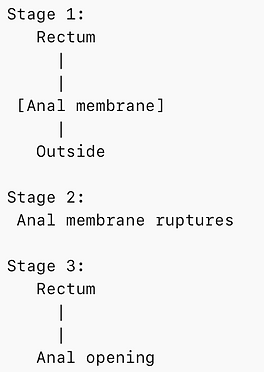
ARM occurs when there is an error in these developmental steps.
Main problems are:
-
abnormal growth of the urorectal septum
-
incomplete separation of cloaca
-
abnormal development of the cloacal membrane
-
failure of anal membrane rupture
-
abnormal development of the perineum

ARM Classifications
2005: International KrickenBeck Classification

1995: Penna Classification of ARM

Wingspread Classification

The most common defect in girls is a rectovestibular fistula followed by a rectoperineal fistula. The third most common defect in girls is persistent cloaca.
The most common defect in boys is a rectourethral fistula, followed by a rectoperineal fistula. Rectobladder neck fistula in boys represent 10% of the entire group.
Imperforate anus without fistula in both boys and girls is unusual and represent only 5% of the entire group of defects, although it is particularly common in patients with Downs Syndrome.
Basic Anatomy & the Continence Mechanism
The anatomical anal canal spans from the anal verge to the dentate line, while the surgical anal canal extends from the anal verge to the anorectal ring. Anorectal ring is a muscular structure at the junction of the rectum and anal canal, formed by the fusion of the internal and external anal sphincters and the puborectalis muscle.


The perineal body serves as a central convergence point where fibers of several muscles interlace and overlap. These include the bulbospongiosus, external anal sphincter, both the superficial and deep transverse perineal muscles, as well as smooth and skeletal muscle strands from the external urethral sphincter, levator ani muscles, and the muscular layers of the rectum.

Continence Mechanism is provided by:
1. Internal anal sphincter - 50-85% of involuntary resting tone
2. External anal sphincter - 20-25% of involuntary resting tone
3. Pubo-rectalis [levator ani]
4. Anal mucosal folds and vascular cushions
5.Anorectal relationship6.Rectum as reservoir - compliance and capacity
7.Nerve Supply and physiology of defecation
8.Pressure differential between rectum [ 6 cm water] and anal canal [90 cm water]
Circular muscles of the rectum continue as the internal anal sphincter, ends below the dentate line and above the external anal sphincter.
Levator ani forms the external anal sphincter, between these two sphincters the longitudinal muscle coat of the rectum thins out to form the conjoint longitudinal muscle, joins some fibers from the puborectalis. Some of the IAS and CLM extend into the submucosa known as the muscle of treitz.


PELVIC FLOOR ANATOMY IN RELATION TO CONTINENCE & ANORECTAL MALFORMATION
The pelvic floor functions as a continence machine made up of three main components: the levator ani muscle complex (LAMC), the external anal sphincter (EAS), and the internal anal sphincter (IAS). Together, these structures support the pelvic organs, maintain the anorectal angle, and provide resting as well as voluntary continence. In anorectal malformations (ARM), these structures may be malformed, hypoplastic, displaced, or poorly aligned, which is why detailed anatomical understanding is essential during posterior sagittal anorectoplasty (PSARP).
The levator ani muscle complex is the most important muscular component for continence. It includes the pubococcygeus, puborectalis, and iliococcygeus. Among these, the puborectalis is the key muscle for continence because it forms a U-shaped sling behind the anorectum and creates the anorectal angle. During continence, it contracts and sharpens this angle, preventing stool leakage; during defecation, it relaxes and allows the angle to straighten. In ARM, the puborectalis is often hypoplastic or displaced, and successful placement of the neo-rectum within this sling is crucial for functional outcome.
The internal anal sphincter (IAS) is a smooth muscle continuation of the rectum and provides most of the resting anal pressure. It is under autonomic control. In ARM, the IAS is often absent or severely underdeveloped, leading to reduced resting tone. The external anal sphincter (EAS) is a voluntary striated muscle supplied by the pudendal nerve (S2–S4). It is responsible for squeeze control, urgency control, and gas continence. In ARM, the EAS may be present but malpositioned, so correct centering of the rectum within the sphincter complex during PSARP is essential.
Continence also depends heavily on nerve supply. The pudendal nerve provides voluntary motor control to the EAS and levator ani and carries somatic sensation. The autonomic nerves regulate IAS tone and colonic motility. In ARM, these nerves may be present but not normally directed, which helps explain why continence outcomes vary even after technically good repairs.
Normal continence depends on an intact anorectal angle, maintained mainly by the puborectalis. During defecation, this muscle relaxes, the angle straightens, the EAS relaxes, and abdominal pressure assists expulsion. If the puborectalis is underdeveloped, angle control is poor and chronic soiling may result.
Different types of ARM have predictable pelvic floor abnormalities. In high ARM, the levator muscles are poorly developed, the rectum ends above the sling, and continence potential is poor. In intermediate ARM, muscle development is better and the rectum lies closer to the sling, so continence is usually better. In low ARM, the levator ani is near normal, the IAS is usually present, and continence potential is generally very good.
During PSARP, the surgeon must identify the midline muscle complex, recognize the puborectalis sling, place the rectum exactly in the center of the sphincter mechanism, and preserve pudendal nerve branches by avoiding wide lateral dissection. Proper placement of the rectum within the muscle complex is one of the most important determinants of continence outcome.
Continence has two major components: muscular continence and sensory continence. Muscular continence depends on the IAS, EAS, and puborectalis. Sensory continence depends on intact anoderm, perianal skin sensation, and the ability to distinguish gas, liquid, and stool. ARM affects both systems, but sensory continence is often even more impaired than muscular continence.
The anoderm is highly specialized sensory tissue below the dentate line, rich in nerve endings and receptors. It plays a key role in the sampling reflex, fine continence, and feedback for voluntary squeeze. The dentate line separates the visceral sensory zone above from the somatic sensory zone below, making it crucial for continence and reflex sphincter activity. In ARM, the dentate line does not develop normally, and the anoderm is often absent or replaced by mucosa. As a result, children may have poor sensation, inability to distinguish gas from stool, absent sampling reflexes, passive soiling, and weak toilet training response even if the sphincters are reconstructed well.
Additional sensory problems arise when the neo-anus is placed off-center or when scarring from surgery reduces skin sensitivity. These factors impair feedback, delay awareness of leakage, and worsen soiling. MRI studies also show that levator ani muscle bulk correlates with continence outcome: high ARM usually has small thin levators, while better muscle bulk is associated with better Krickenbeck continence scores.
Pelvic Diaphragm
Pelvic diaphragm helps maintain fecal continence, supports the pelvic visceras and resist the intraabdominal pressure.
Anterior fibers: Forms a sling and inserts into the perineal body
Intermediate fibers: puborectalis forms sling around the junction of the rectum and the anal canal - maintain the anorectal angle of 80-90 degrees. Pubococcygeus muscle forms the sling and inserts into the annococcygeal body
Posterior fibers: Ileococcygeus inserted into anococcygeus body and coccyx
Nerve Supply: Pudendal nerve S2-S4.
Sphincter Mechanism
Forms a funnel like structures from cranial to caudal direction:
1. Levator muscles: Puborectalis fibers of the levator ani forms the anorectal ring. Its lower border defines the upper extent of high anal canal where it is continuous with the muscle complex. If it is stimulated, it pulls the rectum forward
2. Muscle Complex: It elevates the anus. Vertical group of striated muscle fibers of the deep external sphincter, continuous with the levator ani. Slimulation causes the closure of the anus.
3. Parasaggital Fibers: Subcutaneous part of the external sphincter, surrounds the lower anal canal that runs parallel in axial plane. Closes the anus when stimulated.
Ischial Line
Demarcated at the inferior end of the ischial comma (ossification center of the ischium). It corresponds to the upper surface of the bulb of the urethra in males and the upper limit of the perineal body and level of triangular ligament in females. The anal pit is 1-2cm caudal to the ossified ischium.
The triangle bounded by the PC line and I point denotes the radiographic markings of the levator complex in neonates with significant ARM, with bowel terminating above the sphincter muscle complex.


Distal Colostogram Interpretation
Enables demonstration of the location and length of the blind rectum and the precise site of a rectourinary fistula. The rectum is surrounded by striated muscle, which keeps it collapsed and prevents filling of the most distal part. This may give the erroneous impression of a very high defect and may prevent demonstration of a rectourinary fistula, which is always located at the most distal part of the rectum. To avoid this problem, the contrast medium must be injected with considerable hydrostatic pressure under fluoroscopic control. The use of a Foley catheter is recommended; it is passed through the distal stoma, the balloon is inflated (2–5 mL), and it is pulled back as far as possible to occlude the stoma during the injection of the contrast medium. In cases of rectobladder neck fistula, the surgeon doesn’t expect to find the rectum through the PSARP approach and thus avoids the blind perineal dissection.
The scout film can give information about the fistula by demonstrating air in the bladder. The lateral film can also give information about the status of the spine. The colon can also be inspected for fecal loading.
The distal colostogram must be a 'pressure' colostogram, that means that the blind end of the rectum should be bulging to ensure adequate visualisation of the fistula and should not be flat. Flat colostogram is shown in the picture below:

To enable adequate interpretation of the colostogram, one should be aware of the anatomy of the urinary tract. Three major types of fistulas exist: rectobladder neck, rectoprostatic and rectobulbar urethral fistula.
If we imagine the bladder and the urethra as an arm outpouching from the bladder, we can interpret these findings adequately as shown in the picture below:

The head of the humerus represents the bladder neck, the body of the humerus: rectoprostatic and the elbow and beyond, rectobulbar and rectourethral fistulas. Just note where the distal tapering of the rectum is meeting the urinary tract.

Diagram A represents a rectobulbar urethral fistula and can be approached via the PSARP approach, Diagram B shown a rectoprostatic fistula and may require an additional abdominal approach, diagram C shows a rectobladder neck fistula and will require an abdominal approach.

Draw a PC line (Pubococcygeus line) on the lateral film of the distal colostogram. A helpful anatomical landmark is to mark the pubococcygeal line (PC line), and if the rectum is above that line, an abdominal approach is needed. If the distal rectum is below the line, the rectum is reachable through a posterior sagittal incision. The surgeon must know before starting the operation, whether the rectum is the first anatomical structure encountered from a posterior sagittal approach, and if so, a posterior sagittal approach is best. If the urinary tract would be encountered first via a posterior sagittal incision, laparoscopy (or laparotomy) is needed.
How to explain:
this is most likely a distal loopogram as contrast is seen to be given by the distal stoma. It is deliniating the distal sigmoid and the rectum. The length of the loop seems adequate. the lower end of the rectal pouch is crossing the sacrum and the floor as well (not shelfing on it). Most likely a low lying variety.
Comment on the sacrum, vertebra, no mass infront of the sacrum, count the sacral pieces (the oblique piece is the first sacral vertebra), fecal loading, fistula.
Types of Fistulas
Rectoperineal Fistula
This type of defect is also known as a low imperforate anus. The rectum is located within most of the sphincter mechanism. Only the lowest part of the rectum is anteriorly displaced. Well formed anal dimple and a prominent skin tag in a midline perineal raphe, scrotum or penis (If instrument passed below it then its called a bucket handle deformity). The sphincteric mechanism is very good, and therefore the prognosis is also good.
Rectourethral bublar and prostatic Fistula
The rectum may communicate with the lower part of the urethra (bulbar urethra) or with the upper urethra (prostatic urethra). Immediately above the fistula site, the rectum and urethra share a common wall with no plane of dissection. This anatomic fact has important technical implications. The rectum is surrounded laterally and posteriorly by the levator muscle mechanism. Between the end of the rectum and the perineal skin, there is a portion of striated voluntary muscle called the ‘muscle complex’. The contraction of the levator muscle pushes the rectum forward. The contraction of the muscle complex elevates the skin of the anal dimple. At the level of the skin, and located on both sides of the midline, there is a group of voluntary muscle fibers called ‘parasagittal fibers’. Note ‘normal sacrum’, ‘prominent midline groove’.
Patients with rectourethral prostatic fistulas tend to have an abnormal sacrum, underdeveloped sphincter mechanism, and flat perineum. The anal dimple is often located very close to the scrotum.
Rectobladder Neck Fistula
The levator muscle, muscle complex, and parasagittal fibers are often poorly developed. The sacrum is often deformed or absent.
Imperforate anus without fistula
In these cases, the rectum is completely blind and is almost always found at the same level as in cases with rectourethral bulbar fistula. The sacrum and sphincteric mechanism are usually normal and therefore these patients have a good prognosis.
Rectal atresia/stenosis
1% - Normal appearing anal canal. About 2 cm from the anal verge, there is an atretic or stenotic area. The upper blind rectum is usually located very close to the anal canal. The sacrum is normal, the sphincteric mechanism is excellent, and therefore the prognosis is good. This malformation is particularly associated with a presacral mass.
Rectovestibular fistula
The intestine opens in the vestibule of the female genitalia immediately posterior to the hymen. The most pertinent anatomic characteristic of this defect is that immediately above the fistula site, the rectum and vagina share a very thin common wall. These patients usually have good muscles and a normal sacrum.
H type Anorectal Malformation
An H-type anorectal malformation (ARM) is a rare congenital anomaly featuring a direct connection (fistula) between the rectum and the urogenital tract (vestibule/vagina in females, urethra in males) while a normally located anus is usually present.
A Case:
The patient had passed meconium in the first 24 h of life, but on exam was noted to have a slit-like anus. Particulate matter was also found in the urine. The remainder of the medical history and physical exam was unremarkable. Imaging workup consisted of a renal ultrasound demonstrating debris and air within the bladder. A barium enema was performed to further delineate the anatomy, which demonstrated a colourethral fistula, most likely to the posterior urethra. At two months of age, the patient underwent posterior sagittal anorectoplasty (PSARP) with ligation of the H-type rectourethral fistula (Fig below). The fistula was identified on the anterior wall of the rectum and was quite large and patulous.



Funnel Anus
It is characterized by a funnel-shaped anus which is skin lined and extends up to a stenotic ring where it joins the rectal mucosa abruptly without the intervention of any transitional epithelium. It is characterised by fibrotic, scarred sphincter and a malformed external sphincter.
Management Protocols
Generally we have five challenges in managing a baby with ARM:
1. Save the life (Hypoglycemia, Cardiac anomalies, IV fluids, Airway management)
2. Decision to a colostomy or a perineal operation
3. Management of associated anomalies
4. Definitive procedure
5. Bowel management
Males
Intravenous Fluids, NG tube, place a piece of gauze at the tip of the penis, nurse instructed to check the particles of meconium filtered through this gauze.
After 20-24 hours, perform a cross table lateral film performed in a prone position - mark the anal dimple with radio-opaque material. If the patient is growing well and has no other associated defects (cardiovascular or gastrointestinal) that require treatment, he is readmitted at one to three months of age for a posterior sagittal anorectoplasty
Performing the definitive repair at that young age has important advantages for the patient, including less time with an abdominal stoma, less size discrepancy between proximal and distal stoma at the time of colostomy closure, simpler anal dilatation, and no recognizable psychologic sequelae from painful perineal maneuvers. In addition, at least theoretically, placing the rectum in the right location early in life may be an advantage in terms of acquired local sensation. However, diagnostic tests (other than a distal colostogram which obviously requires the presence of a colostomy), used to determine the level of the defect, are not accurate enough, and the surgeon is actually subjecting the patient to a blind exploration of the perineum. If the rectum is located high in the abdomen, the surgeon may damage other structures during the search for the rectum. Such structures include the posterior urethra, seminal vesicles, vas deferens, and ectopic ureters. In addition, there is a risk of dehiscence and infection because the stool is not diverted.

Females
A rectoperineal fistula is the simplest defect in the spectrum of female malformations. These patients can be treated with a minimal posterior sagittal anoplasty, without a colostomy, during the neonatal period.

Choice of a Colostomy
A descending colostomy with separated stomas is preferable for the management of anorectal malformations. The stomas should be separated enough to allow the use of a stoma bag, which covers only the functional stoma.
Transverse colostomies have several disadvantages: the mechanical preparation of the distal colon before the definitive repair is much more difficult and, in the case of a large rectourethral fistula or rectobladder fistula, the patient often passes urine into the colon, where it remains and is absorbed, leading to metabolic acidosis. Also, during the distal colostography, it is more difficult to distend the distal rectum and define the anatomy. Patients with transverse colostomies are more likely to develop a megarectosigmoid.
Procedures
Rectovestibular Fistulas in Females
At birth, the patient can be put on dilatations and a definitive procedure (ASARP) can be performed at 3-4 months of age with or without a diverting colostomy
Distal Rectum <2cm from the proposed anal site or below the level of the coccyx on the lateral cross table view at birth
Primary Anoplasty with or without a colostomy can be performed. The patient is placed in a lithotomy position and a cruciate incision is given after anal mapping within the sphincter. After encountering the rectum, it is checked by aspirating with a 10cc syringe. If meconium is encountered, then make a cruciate incision on the rectum opposite to the incision on the skin so that both incisions interdigitate. The patient is then put on dilatations

Distal Rectum >2cm from the proposed anal site or above the level of the coccyx on the lateral cross table view
Colostomy at birth and PSARP at 6 months of age.
Posterior Saggital Anorectoplasty
-
Position: The patient is placed in the prone jackknife position under general anesthesia - request the anaesthetist not to give a muscle relaxant until anal mapping is done.
-
Preparation: The perineum is cleaned, draped, and the anal dimple is identified.
-
Incision: A midline posterior sagittal incision is made from the middle of sacrum toward the anal sphincter.
-
Foley's Catheter: A foley's catheter is inserted in the urethra, this catheter can go in the rectum rather than the urethra, to avoid this a coude's catheter is used that is directed anteriorly. Cystoscopic insertion of a catheter over a glidewire is another option.
-
Midline dissection: The skin, subcutaneous tissue, and muscle are divided strictly in the midline.
-
Muscle identification: The external sphincter and levator muscle complex are identified, often using a muscle stimulator. The fibers of the muscle complex run perpendicularly and medial to the parasagittal fibers. The lavator ani muscles lie deep in the incision are then divided (they are parallel to the skin inicison) in the midline exposing the rectal pouch.
-
Exposure of rectal pouch: The rectal pouch is carefully dissected and exposed. Two silk sutures are placed in the posterior rectal wall on both sides of the midline. The rectum is opened between the sutures and the incision is continued distally exactly in the midline down to the fistula site.
-
Fistula management: Any rectourethral fistula is identified, ligated, and divided. A plane of seperation is created in the common wall. Multiple 6/0 PDS sutures are placed through the rectal mucosa immediately above the fistula in a semi circle. The rectum is then seperated from the urethra creating a submucosal plane for approximately 5-10mm above the fistula site until the rectum is freed from its adherence to the periurethral tissue.
-
Rectal mobilization: The rectum is mobilized adequately while preserving its blood supply. Remain within the whitish fascia to avoid damage to the innervation of the bladder and the genitilia.
-
Creation of pull-through path: A channel is made through the center of the muscle complex.
-
Pull-through: The rectum is pulled down through the center of the sphincter mechanism. The posterior limit of the muscle complex must also be reapproximated behind the rectum. Inclide the rectal wall to anchor it to avoid prolapse.
-
Positioning: The bowel is positioned accurately within the levator and sphincter complex.
-
Anoplasty: A neoanus is created at the site of the normal anus.
-
Calibration: The neoanus is calibrated to an appropriate size.
-
Closure: The muscle complex and wound are closed in layers.
-
Postoperative care: Hemostasis is ensured, dressing is applied, and later anal dilatation is started as planned.
Aims/Goals:
-
Create a functional anus in the centre of the sphincter muscle complex
-
Establish normal anatomy of anorectal structures with a straight tension free rectal pull through
-
Preserve continence mechanism
-
Safely identify and seperate rectum from the urogenital tract preventing urethral or vaginal injury
-
Close any fistula securely
-
Achieve good cosmetic and functional outcome for long term bowel control
-
Prevent complications such as stricture, retraction, recurrent fistula and incontinence
Principles:
-
Strict midline dissection that is avascular and safer
-
Identification of sphincter mechanism using a nerve stimulator
-
Preservation of all continence muscles
-
Adequate rectal mobilisation
-
Straight alignment appropriate neoanus construction with a circular mucocutaneous anastomosis with an appropriate diameter to avoid stenosis or incontinence
-
Minimal tissue trauma and meticulous dissection
Complications
Wound infections
Anal stenosis due to ischemia (check for bleeding margins)
Constipation (more in lower malformations)
Transient femoral nerve pressure (due to jack knife position)
Neurogenic bladder due to absent sacrum, tethered cord or nerve damage during PSARP
Retraction: Check for free lie over the anal verge
Prolapse: posterior midline tagging. If prolapse exists then differentiate between partial and complete prolapse, if partial then do local resection and stitches or injection sclerotherapy. If complete, then redo operation and tag rectum to the posterior waldayer's fascia. Can also do MRI to detect hypoplasia of muscles.
Layers Encountered During PSARP
-
Skin: An incision is made in the mid-sacrum, extending to the anal dimple.
-
Subcutaneous Tissue/Fat: Layers of fat beneath the skin.
-
Fascial Layer: The superficial fascia.
-
Striated Muscle Complex: This is the most crucial layer, which includes the external anal sphincter, the levator ani muscle (pubococcygeal and iliococcygeal portions), and the puborectalis muscle. These muscles are split in the midline using electrostimulation to ensure precise identification.
-
Perirectal Fat: Fatty tissue surrounding the rectum.
-
Rectal Pouch/Fistula: The blind-ending rectum is identified, dissected, and freed from surrounding structures (such as the urethra, bladder, or vagina).
Follow up
The Foley catheter is left in place for 7 days. The patient receives broad-spectrum antibiotics for 1 day and prophylactic antibiotics while the Foley is in place.
Two weeks after the operations, anal dilatations are started. On the first occasion, a dilator that fits loosely into the anus is used to instruct the parents, who must carry out dilatation twice daily. Every week, the size of the dilator is increased until the rectum reaches the desired size, which depends on the patient’s age. Once the desired size is reached, the colostomy can be closed. The frequency of dilatations may be reduced once the dilator of desired size passes easily. This reduction should occur according to the following schedule: at least once a day for one month; every third day for one month; twice a week for one month; once a week for one month; and every 2 weeks for three months.
. A baby who has one to three bowel movements each day, remains clean between bowel movements, and pushes during each bowel movement (indicating that there is some feeling during the defecation process) has, in general, a good functional prognosis, and therefore is likely to respond to toilet training.
How to Callibrate Hegar’s Dilators?
First dilatation should be done under GA, do nerve stimulation, set the number, teach mother and make sure they cross the sphincter and keep it in for 30sec. Dilators curvature should be in the shape of the sacrum.




Abdominal Approach If needed in cases of rectovestibular/rectobladder neck or rectoprostatic fistulas
-
The abdomen is entered either via laparotomy or laparoscopically, and the rectosigmoid colon is mobilized. The peritoneum should be divided around the distal rectum to create a plane of dissection to be followed distally. The dissection should stay right on the rectal wall. At the point where the rectum becomes narrow, where it communicates with the bladderneck, it should be divided.
-
The bladder side of the fistula should be sutured or ligated with an endoloop
-
The rectum communicates with the urinary tract in a T fashion, which means that there is a minimal common wall between the distal part of the rectum and the urinary tract. The surgeon must be careful to avoid damage to the vas deferens, which run very close to the bowel
-
Ligation of the inferior mesenteric vessels as high as possible, very close to their origin near the aorta, would mobilize the rectum, but would probably compromise the blood supply of the rectum because the arcades that connect the middle colic vessels with the inferior mesenteric ones may have been interrupted at the time of the colostomy creation. Instead, the surgeon must ligate the most distal branches of the inferior mesenteric vessels close to the rectum. If this is done, the more proximal branches of the inferior mesenteric vessels must be left intact to guarantee a good blood supply which runs intramurally to the rectum. A tapering of the distal dilated rectum can also increase length.
-
At this point with the legs lifted, a small perineal mid-sagittal incision is performed. The presacral space is dissected (a mosquito clamp dissects gently along the curve of the sacrum) and is visualized through the abdomen. The rectum is pulled through. Great care is taken to avoid urethral injury, as the course of the urethra is directly in front of the course of the future pull-through.
The Future
Robotic assistance (RAARP) is emerging. New single-center series and propensity-matched analyses (2024–2025) suggest feasibility and potential perks (less blood loss, shorter stay/OR time) vs. LAARP—evidence is early and numbers are small, so treat as evolving rather than standard.
Anal sphincter augmentation after PSARP/LAARP (post-ARM incontinence): small pediatric projects and proposals use mesenchymal/adipose-derived cells or myoblasts injected into the anal sphincter to improve squeeze/function.
Fuctional Disorders after Repair
-
Deficiencies in Sensation: This means that they do not have the exquisite sensation that normally resides in this anatomic area. Most patients, however, still preserve a vague sensation called proprioception, generated from distension of the rectum, and therefore stretching of the voluntary muscles around it. Liquid stools, which do not distend the rectum, are not felt by most of these patients.
-
Defective Sphincter Mechanism
-
Coordinated Rectosigmoid motility: This constipation seems to be more severe in patients with lower defects. An ectatic distended colon (sometimes associated with a loop or transverse colostomy) leads to megarectosigmoid and eventually provokes severe constipation.
Management of Fecal Incontinence
Bowel management Program
Training the parents and children to clean out the colon once daily with the use of enemas and to avoid bowel movements between irrigations by adherence to specific diets and sometimes medications. Socially acceptable members of the society. To be a functioning member of the society
Contrast enema/Defecography, VCUG, MRI Spine and Pelvis (for muscle status). Divided into two groups:

Acute Urinary retention after removal of foleys after 7 days:
-
Can result from
-
pain
-
pelvic edema and low grade ongoing infection
-
Urethral injury
-
Preoperative neuropathic bladder that was not managed/diagnosed preoperatively
-
Damage to pelvic splanchnic nerves
Management:
Adequate pain control → Place the child in luke warm water and instruct to urinate in the bath → try to pass a urinary catheter → do a cystoscopy to rule out mechanical obstruction → Urodynamic studies can be done in as little as 3 months → get an MRI for spinal dysriaphism → leave catheter for 10 days and give a trial (ask if there’s peritubal leakage) → give alpha blockers If unable to pass catheter then place a suprapubic catheter.
SOILING AND POOR CONTROL AFTER ARM SURGERY
Causes: (1)Absence of anal skin and canal in high variety ARM, there are no sensations and variable proprioception (2) Anteriorly placed anus out of the sphincter complex (3)Sacral Agenesis (4) Neuropathic - Poor internal anal sphincter complex (5) Weak pelvic muscles (6) Absence of rectosigmoid - No reservoir capacity (7) Overflow incontinence
Counselling: Nature of problem, Dietary Modifications, Irrigation by Saline enemas, Toilet training (routine after major meal), Pelvic floor exercises, Emotional support and commitment of parents, Abnormal position of rectum and anus, re-operation and placement of rectum within the sphincter complex.
↓
Malone Antegrade Colonic Enema → Continent Stoma, irrigation with soap, polyethylene glycol solution glycerine
↓
Colostomy
For constipation: Diet-Bran, Fruit juices, vegetable, water, laxatives, large saline enemas, behavorial modifications (Toilet training, Evacuation Diary), Malone antegrade enema → Not responding → Colostomy
For Increased motility: Constipating diet: Apple Juice, Banana, Rice, Milk, White bread, Loperamide.

ALGORITHM
Position of Anus
Sphincter Squeeze
Fecal Impaction
Sacral agenesis
Lipoma
Spina Bifida
↓
X ray (Fecal Impaction, Presacral mass, mass effect, Sacral/Vertebral anomaly)
↓
Water soluble contrast enema —> Distension of colon, stricture, presacral mass effect
↓
MRI Spine/Pelvis → Tethering of Spinal Cord
↓
USG KUB
↓
Radioisotope colonic motility transit times to assess for colonic motility
↓
Anorectal manometry to assess for sphincter complex
↓
Parental Counselling
↓


Persistent Cloaca
-
Rectum, vagina, and urethra are fused into a single common channel. Treatments traditionally involved repair of the rectal component of the malformation, leaving the urogenital sinus alone, planning its repair in a second stage, or performing a combined abdominoperineal approach with vaginal and rectal pull-through.
-
Length of the common channel varies from 1cm to 10cm. When the common channel is shorter than 3 cm, patients usually have a well-developed sacrum and good sphincters. When the common channel is longer than 3 cm, this usually suggests a more complex defect and the patient often has a poor sphincter mechanism and poor sacrum.
-
These patients often have small external genitalia. Sometimes patients with cloacas have a palpable lower abdominal mass that represents a distended vagina (hydrocolpos).
-
Perform a rapid urological evaluation → Abdominal ultrasonography to rule out hydronephrosis/hydroureter and/or hydrocolpos. In 30 percent of these cases, the vagina is abnormally distended and full of urine and mucous (hydrocolpos). The distended vagina may compress the trigone, interfere with the drainage of the ureters, and produce megaureters.
-
The vagina and uterus commonly show varying degrees of septation. The rectum usually opens in between the two hemivaginas.
-
Some of these patients may also suffer from cervical or vaginal atresias or stenoses. When undetected, these may interfere with the drainage of menstrual blood during puberty
-
All babies with a cloaca need a colostomy. It is important to perform the colostomy proximally enough to avoid it interfering with the repair of the malformation (pull through and possible vaginal replacement).
-
During the opening of the colostomy, it is mandatory to drain the hydrocolpos when present. Can be done transabdominally as well as through the abdominal wall. The indwelling catheter needs to stay in place till the main repair. If two hemivaginas are present, one can make a window between the septum to ensure both are draining adequately.
-
On rare occasions, patients with cloaca are unable to empty their bladders because they suffer from a near-atresia of the common channel. In such circumstances, the baby may require a vesicostomy or a suprapubic cystostomy
-
After the patient has recovered from the colostomy, a high-pressure distal colostogram and injection of contrast through the single perineal orifice will help define the cloacal anatomy. It can demonstrate anatomy as well as assess for VUR.
-
Difference between TUM and PUM is the division of the pubourethral ligament (which gives an additional 2-3cm in length)

Procedure (Posterior sagittal anorectal vaginal urethral plasty (PSARVUP)):
Endoscopy: Endoscopy is recommended to determine the anatomy. This is ideally done outside the newborn period during a separate anesthetic after the patient has recovered from the initial colostomy and/or drainage of a hydrocolpos. The specific purpose of this procedure is to determine the length of the common channel, the status of the bladderneck, and the presence or absence of one or two vaginas and cervices.
Aim:
Separate the rectum from the vagina and place it in the sphincter mechanism
Mobilise the urethra and the vagina so that each is a separate orifice in the perineum.
Reconstruction of urethra, vagina, and rectum, and the achievement of bowel control, urinary control, and sexual function
Cloacas with a common channel length of less than 3cm
Position: Prone position with pelvis slightly elevated
Perform nerve stimulation and do anal mapping
-
With the patient in the prone position, a long midsagittal incision is performed that extends from the middle portion of the sacrum through the sphincter mechanism and down into the single perineal opening. All of the muscle structures are divided in the midline.
-
The incision is continued all the way down to the single perineal orifice, exposing the entire malformation. The entire sphincter mechanism is divided in the midline.
-
The first visceral structure to be found is usually the rectum. Measure perop common channel length.
-
Mobilize the entire urogenital sinus (vagina and urethra together, i.e. urogenital mobilization), as well as the rectum
-
The rectum is opened in the midline and silk stitches are placed along the edges of the posterior rectal wall. The incision is extended distally through the posterior wall of the common channel
-
The next step consists of separating the rectum from the vagina.Rectum and vagina share a common wall.
-
Once the rectum has been completely separated from the vagina, the total urogenital mobilization can be performed. This maneuver consists of the mobilization of both the vagina and urethra as a unit without separating one from the other.
-
The urogenital sinus is transected full thickness between the last row of silk stitches and the clitoris, taking advantage of the fact that there is a natural plane between it and the pubis. Working in a bloodless field, one can very rapidly reach the upper edge of the pubis, where an avascular structure (the suspensory ligaments of the urethra and bladder) can be identified. these ligaments are divided, which immediately provides significant mobilization of the urogenital sinus. With this maneuver, one can gain between 2 and 3 cm of length
-
Dissect the lateral and dorsal walls of the vagina.
-
What used to be the common channel is divided in the midline, creating two lateral flaps that are sutured to the skin of the patient’s new labia. The vaginal edges are mobilized to reach the skin to create the introitus. The limits of the sphincter are electrically determined. The perineal body is reconstructed, bringing together the anterior limit of the sphincter. The rectum is then placed within the limits of the sphincter.
Cloacas with a common channel length of greater than 3cm
-
The rectum is separated from the vagina and urethra. A very long common channel (more than 5 cm) cannot be repaired by total urogenital mobilization alone, and therefore the channel should be left in place so that it can be used later for intermittent catheterization. In this situation, an attempt should be made to separate the vagina from the urinary tract first from below and then from the abdomen by placing multiple 6/0 silk stitches that take the vaginal wall to try to create a plane of dissection between the vagina and the urinary tract.
-
A midline laparotomy is recommended; the bladder is opened in the midline and feeding tubes are placed into the ureters to protect them. A long common wall between the vagina and the bladder exists, and both the ureters run through this common wall. The ureters sometimes have to be skeletonized during this separation and therefore require protection.
-
Once in the abdomen, the patency of the Müllerian structures can be confirmed by passing a No. 3 feeding tube through the fimbriae of the Fallopian tubes and injecting saline solution. If one of the systems is not patent, we recommend its excision, with very careful attention being paid to avoiding damage to the blood supply of the ovary.
-
The procedure continues with the placement of traction sutures in the single uterus or in both hemiuteri. Traction sutures are also placed in the dome of the bladder. With the use of traction on both structures, dissection is initiated between the urinary tract and the vagina. This dissection is continued all the way down to meet the previous dissection initiated from below.
-
The vagina is thus separated from the urinary tract, with care being taken to preserve its blood supply from the uterine vessels
-
The vagina at this point may reach the perineum. If it is found to be too short, some form of vaginal replacement or vaginoplasty is required.
Complications:
Untreated hydrocolpos: The dilated vagina can also become infected, which is called ‘pyocolpos’ and may lead to vaginal perforation and peritonitis.
Prognosis
Low cloacal malformations (less than 3 cm common channel) are usually associated with a well-developed sacrum, a normal appearing perineum, and adequate muscles and nerves. Therefore, a good functional prognosis is expected.
Summary of Procedures:
Common Channel <3cm
Total Urogenital Mobilization. In cloacal anomalies with the common channel less than 3cm in length, the repair includes a maneuver called Total Urogenital Mobilization. For this procedure, we use a posterior-sagittal approach. This means that we make an incision through the middle of the buttocks.
First, we separate the rectum. Next, the urethra and vagina must be mobilized together. For that, we release the suspensory ligament of the urethra, located right behind the public bone. Once free, the urethra and vagina can reach the perineum. The excessive common channel becomes the labia.
Common Channel of Intermediate Length 3-5cm
PSARVUP for repair of cloaca with intermediate common channel Cloaca patients with an intermediate common channel have a channel length between 3 and 5 centimeters , for these patients we use a posterior sagittal approach this means that we make an incision through the middle of the buttocks first we separate the rectum next we try to mobilize urethra and vagina together by releasing the suspensory ligament of the urethra, if the urethra and vagina are unable to reach the perineum we will bring them inside the abdomen to be separated, to do that we open the bladder and catheterise the ureters, we can then separate the urethra and vagina which should now be able to reach the perineum, finally we place the rectum in the center of the sphincter and reconstruct the perinium.
Common Channel that is long >5cm
PSARVUP for the repair of cloaca with long common channel.
For cloacas with a very long common channel, more than 5 cm in length, the separation of structures happens through the abdomen. A foley catheter is inserted into the common channel, and the common channel is left intact as the urethra. The rectum is separated, as well as the hemivaginas, from the bladder. Their insertion is at the same area where the ureters are located. After that, it’s not uncommon that the bladder neck needs to be reconstructed. Many patients will need a partial vaginal replacement since the vagina is located so high in the abdomen that is does not reach the perineum. The blood supply of the colon is carefully analyzed to select a proper piece of bowel that will serve as the partial vaginal replacement. The selected piece of colon is connected to the native vagina. Finally, the rectum is placed in the center of the sphincter.
Vaginal Switch
vaginal switch when cloaca patients have a long common channel into Hema vaginas high in the pelvis
We can perform a maneuver called vaginal switch for this procedure we use a posterior sagittal and an abdominal approach if the rectum is reachable we separate it from the genital urinary tract, next we mobilize the urethra in vagina by releasing the suspensory ligament of the urethra, we then separate the vagina from the urinary tract through the abdomen, at this point the Hemi vaginas are still too high in the pelvis and must be lowered, to do this we take the blood supply of one Hemi vagina and one Hemi uterus, we tubularise the remaining structure which now works as a single vagina, this new vagina is now long enough to switch down to the perineum. Preservation of the blood supply of the ovary is the key.



